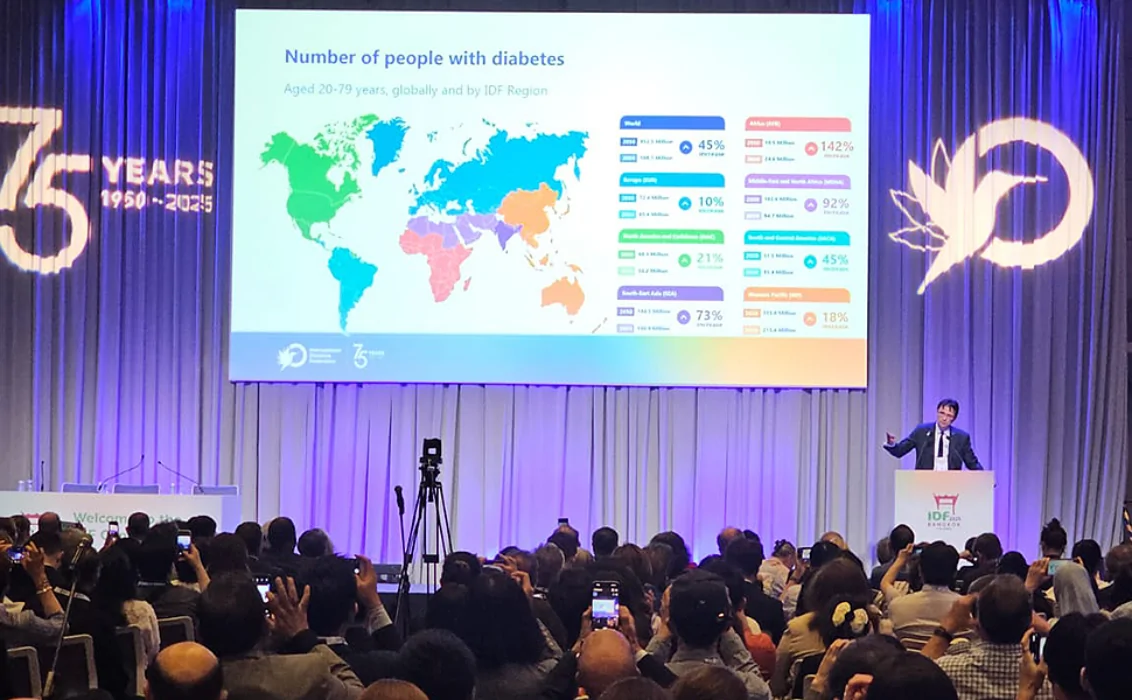
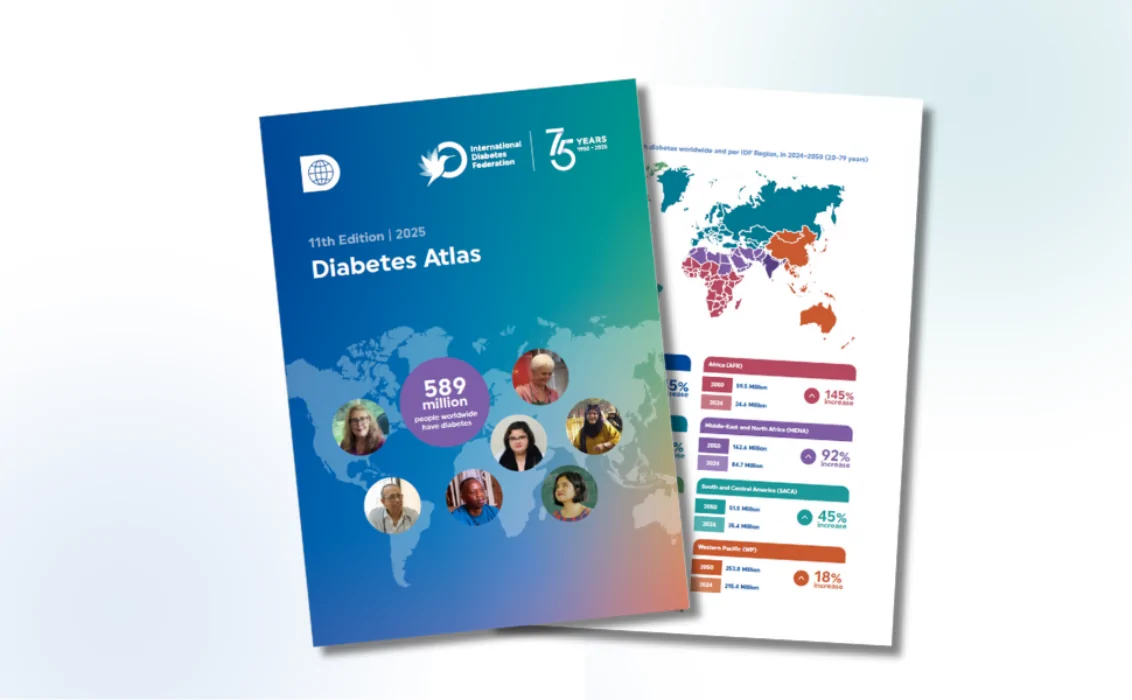
1 in 9 people are living with diabetes
Our mission is to improve the lives of people living with diabetes and prevent diabetes in those at risk.
Our mission is to improve the lives of people living with diabetes and prevent diabetes in those at risk.
Through coordinated advocacy at the global level and at the national level through our members, IDF works to effect change for the millions of people living with diabetes.
IDF awareness activities aim to keep diabetes firmly in the public spotlight and promote the importance of coordinated and concerted action to tackle the impact of the condition.

IDF education initiatives aim to support the development of health professionals and improve understanding of the condition among people living with diabetes.
Notifications